
April 28, 2017 FiDA highlight
Kim Blieschke had no idea her life would change irreparably when she was advised to undergo a “straightforward” surgery to correct pelvic organ prolapse – a complication from childbirth that results in surrounding organs to bulge or sag down into the vagina.
But moments after waking up from her transvaginal mesh implant procedure in 2006, where a web of polypropylene plastic was embedded into her vaginal wall, the mum-of-four knew “something wasn’t quite right”.

“I was in intense pain that they couldn’t control,” Kim told me over the phone from her Port Pirie home, in the South Australian countryside.
“I woke up with quite substantial bruising all over my buttocks and perineum and upper thighs. The bruises were the size of my hand.”
"I had necrotic flesh in there." (Image supplied)
"It was a pain like you wouldn't believe," she said. "Doctors said I'd be in the hospital for two or three days, but I was there for seven. On the three-hour car ride home, sitting was almost unbearable."
From there, Kim's condition spiralled.
"My doctor kept saying it will be better, it will be better, but I ended up taking three months off work," she told me. "I couldn't drive, I couldn't lift, I couldn't even sweep the floor."
Doctors made Kim feel like she was imagining the pain, but as a seasoned paramedic, she knew something was awry when her vagina developed a "foul smell".
"I told my GP something wasn't quite right, and it turned out I had necrotic flesh in there."
The polypropylene - a material used to create everything from plastic chairs to water bottles - had ignited Kim's natural foreign body reaction. Her body wasn't just trying to fight the mesh, it was trying to kill it.
The Therapeutic Goods Administration says transvaginal meshes were approved by "conformity assessment certification either from a EU certification body or the TGA".
By 2014 the TGA admitted its assessment process for the mesh was not “mature” and lacked “rigour”, and subsequently announced there was “little evidence to support the overall effectiveness of these surgical meshes as a class of products”.
By 2015 - a decade after mesh was first approved for embedding within the vaginas of thousands of Australian women - 72 of the 100 mesh products on the Australian market were delisted.
Despite this, where the TGA acknowledged shortcomings of the devices, it mostly blamed "the skill and training of the surgeon and the patient selection".
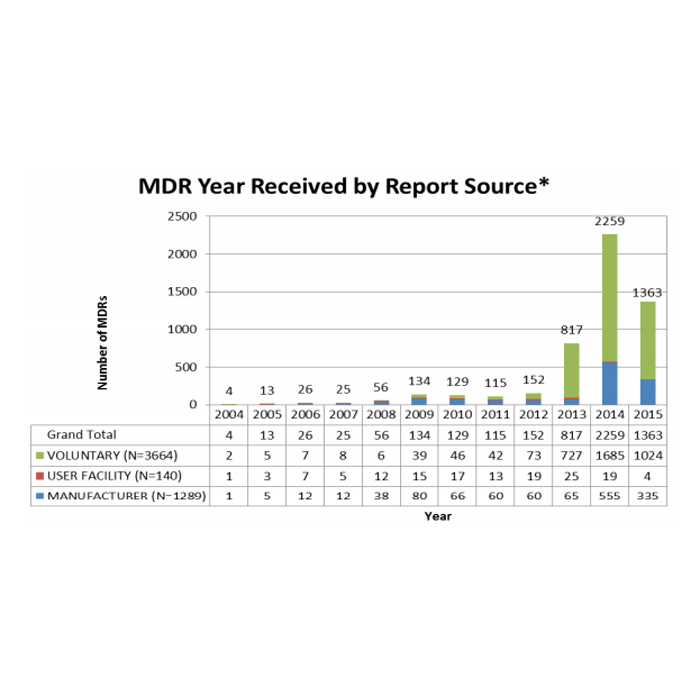
While the TGA said in a statement to Channel 10 it has only received 205 adverse event reports, and "the reported rate of complications was low", Kim argues this is because the channels of reporting post-surgical problems is convoluted and lacks transparency.
The implant that Kim was told to not worry about, the one she was told was simple and straight forward, was eroding away, and destroying her body with it.
"I felt like I was rotting from the inside," she describes.
By the time 2013 rolled around - some seven years after Kim's surgery - her surgeon had retired. The South Australian mum had developed chronic nerve damage which consumed her right hip, knee and two of her toes.
The fetid mesh was deeply affecting her sex life with longterm partner Jared, too.
"When I had intimate relations with my partner, he could feel the hard and brittle arms of my implant against him. It was unbearable.
"A lot of women's partners and husbands have just walked away and left them because of the impact it has on their sex lives, but thankfully my partner has been wonderfully supportive."
The "disastrous" effect the mesh has had has seen Kim spend "hundreds of thousands of dollars", take months at a time off work, and use up all of her long service leave just to find some relief from the constant pain.
Because the real clincher is this: While Australian surgeons are more than happy to insert mesh into women's pelvic floors, they're not so willing to remove it. In fact, there are only two doctors in the world who offer to take out transvaginal mesh, and both live in the United States.
To have the toxic mesh removed requires a six-month stint off work to visit the US, and an upfront payment of $50,000, something Kim pursued and succeeded with.

There are only two doctors in the world who offer to take out transvaginal mesh. (Image supplied)
While the mesh might be out of her body, the havoc it wreaked is irreversible and will stay with Kim forever.
"My mesh was embedded in my bowel, my rectum, and my urethra," Kim told me. "Now, my whole pelvic floor is just a massive scar tissue. I am now incontinent, my nerve damage and muscle damage is permanent, and I live on medications."
Kim also lives with a level of anxiety she likens to post traumatic stress disorder.
"I'm certainly not the woman and I am not the mother I once was," she said. "I feel like I've lost a big part of myself. I can't be with my kids as much as I'd like, I can't play or do all the things I wanted to do with them. There are some days when I can't get out of bed."
If there is any solace in this tragedy, it's that Kim Blieschke can find comfort in the other Australian women who have also lived this hell. In fact, hundreds have reported serious health complications as a result of transvaginal mesh implants to the TGA, and a medical review predicts there are 4000 more silently suffering in the shadows behind them.
When Kim found someone who had experienced what she had online, she was overwhelmed.
"I just burst into tears because I honestly thought that I was on my own," she said. "I was told that it was all in my head, and to find that there was someone else, and for all these women to come forward was incredible.
 "It's something that nobody really wants to talk about because people feel embarrassed, but as far as I'm concerned I want everyone to know about it."
"It's something that nobody really wants to talk about because people feel embarrassed, but as far as I'm concerned I want everyone to know about it."
"I want everyone to know about it." (Image supplied)
Kim is now one of the handful of women who are leading the charge to have transvaginal mesh implants banned. Her meeting with Victorian Senator Derryn Hinch last year proved pivotal in pushing discussion forward about what Hinch describes as "one of the greatest medical scandals and abuses of mothers in Australia's history".
It falls in line with the opinion of The Royal Australian and New Zealand College of Obstetricians and Gynaecologists, who state that "very little robust information is available on the efficacy and long term safety" of polypropylene mesh to treat pelvic organ prolapse, warning women of "adverse" effects.
Thanks to women like Kim, and Senator Hinch, there is now a Senate inquiry into the mesh, which has a reporting date of November 30.
But the aim is to do more than just have the mesh banned - it's to get justice.
"We would like someone to be answerable to this," Kim explained. "Because none of the surgeons are mandated to report the complications, they don't. We want women to have informed consent, because a lot of women are just told this is a straight forward operation when it's not, it can ruin lives."
And on behalf of Mamamia, we dearly hope Kim, and the many women beside her, succeed.
If you are a victim of transvaginal implants, Mamamia encourages you to lodge a complaint by clicking on your state:
Victoria; New South Wales/ACT; Queensland; South Australia; Western Australia; Tasmania; Northern Territory.
http://www.mamamia.com.au/transvaginal-mesh-implants/







































{kind=link}