
Showing posts with label MAUDE. Show all posts
Showing posts with label MAUDE. Show all posts
Monday, November 20, 2017
Thursday, May 25, 2017
Dr. Amy Reed Dies at Age 44, Mother of 6 Children and Advocate for Safe Medical Devices
By DENISE GRADY
MAY 24, 2017 (FiDA highlight)
Dr. Amy J. Reed, a physician and cancer patient who turned a personal calamity into a crusade to spare other women from the medical procedure that harmed her, died on Wednesday night at home in Yardley, Pa. She was 44.

Dr. Amy J. Reed and her husband, Dr. Hooman Noorchashm, in 2014. (MATTHEW CAVANAUGH FOR THE NEW YORK TIMES)
Her husband, Dr. Hooman Noorchashm, said the cause was leiomyosarcoma of the uterus, a type of cancer.
Dr. Reed and her husband fought for years to ban the use of a surgical tool called a power morcellator, which has a spinning blade that slices up tissue so it can be extracted through small incisions. Though the device is regarded as a great boon to minimally invasive surgery, if a patient has cancer, as Dr. Reed did, morcellation can spread the disease.
Dr. Reed and Dr. Noorchashm (pronounced NOOR-chasm) won some notable victories. Because of their efforts, the Food and Drug Administration studied morcellation and in 2014 recommended that it not be used in the “the vast majority” of women having surgery for uterine fibroids, a common tumor that is usually benign but that can hide a dangerous type of cancer.
Some insurers began declining coverage for morcellation, and one major manufacturer took its morcellators off the market. Use of the technique dropped.
Dr. Reed, an anesthesiologist and the mother of six children, underwent surgery involving morcellation in 2013, when, at 40, she had her uterus removed because of fibroids. The operation was performed at Brigham and Women’s Hospital in Boston, which is affiliated with Harvard Medical School, where both Dr. Reed and Dr. Noorchashm had teaching positions. A biopsy after the operation found that Dr. Reed had a hidden leiomyosarcoma, an aggressive type of cancer.
Only then were Dr. Reed and her husband told that her surgeon had used a power morcellator to slice up her uterus. The device allows doctors to work through small slits rather than big, open incisions, so that patients can heal faster and run less risk of bleeding and infection.
At that time, morcellation was performed on 50,000 women a year in the United States to help remove fibroids, or to remove the entire uterus.
The device had sprayed malignant cells around inside Dr. Reed’s abdomen, leaving her with an advanced, Stage 4 cancer.
As physicians, Dr. Reed and Dr. Noorchashm knew at the time that her morcellation procedure could be a death sentence. As a surgeon himself, Dr.
Dr. Reed quickly embarked on a series of aggressive treatments, but she still suffered one recurrence after another, in her abdomen, lungs and spine. She had several major operations and received arduous courses of chemotherapy, radiation, immunotherapy and experimental treatment.
The couple fought the medical establishment as fiercely as they did the cancer, seeking to ban morcellation. They sent thousands of emails to the F.D.A., device makers, hospitals, legislators, professional societies and individual doctors, and they reached out to news organizations to publicize their cause.
Dr. Noorchashm also collected the names and histories of women whose cancer had spread after morcellation, enlisting them, or their survivors, in the crusade.

Dr. Amy Reed with her husband, Dr. Hooman Noorchashm, and their children in their backyard in Yardley, Pa., in the summer of 2015.
JENNIFER CAPOZZOLA
Their activism, alienating some colleagues and aggravating administrators, came at a price. Dr. Noorchashm had been a rising star in cardiothoracic surgery at Brigham and Women’s, where his wife had the operation, but as he continued to criticize its gynecology department, his career there began to stall.
He and Dr. Reed were both hired by the University of Pennsylvania, and moved there in 2014. Both had extended family in and around Philadelphia.
They had apparently burned their bridges at Harvard. At one point, when Dr. Reed needed to return to Brigham and Women’s for a medical procedure, she and Dr. Noorchashm were stunned to find that the hospital had assigned a guard to inspect their bags and escort them at all times, for security reasons. Dr. Noorchashm called a lawyer. A judge put a stop to the escort, issuing a restraining order against the hospital.
The gynecology profession also fought back against Dr. Noorchashm and Dr. Reed, insisting that leiomyosarcoma was so rare that the benefit of morcellation — the ability to have minimally invasive surgery — far outweighed any risk.
Before 2013, the F.D.A. had received no reports of uterine cancers being spread by morcellators. But after Dr. Reed and her husband went public — interviewed by newspapers, magazines and TV news shows — reports began to pour in. Dr. Reed, with her hair gone and her youngest child sometimes climbing onto her lap during interviews, was a sympathetic figure.
The couple’s efforts gained traction. The F.D.A. responded by studying published and unpublished medical data on morcellation. Before then, estimates of how many women with fibroids would have undiagnosed leiomyosarcomas or other uterine sarcomas were based on studies of varying reliability, and ranged from 1 in 10,000 to in 1 in 500. But the F.D.A. concluded in April 2014 that hidden sarcomas were more common than earlier estimates had stated — and probably occurred in about one in 350 women with fibroids. The tumors are extremely difficult to detect without surgery.
Soon after the F.D.A. issued its findings, one maker of morcellators, Johnson & Johnson, pulled its devices off the market. But others remained.
In November 2014, the F.D.A. went further, recommending that power morcellators not be used in the vast majority of women having fibroid surgery. Using the device in women with undetected sarcomas, it said, “may spread cancer and decrease the long-term survival of patients.” The F.D.A. portrayed the statement as a “safety communication,” not as an announcement of a new regulation.
Morcellator use dropped significantly, but many gynecologists still favored it, and the devices remained available. Dr. Noorchashm and Dr. Reed would not settle for less than a complete ban, and continued to agitate. They prodded legislators to ask the Government Accountability Office to investigate morcellation.
In a report issued in February, the G.A.O. criticized the F.D.A.’s method of collecting data on problems stemming from morcellation, noting that the system was dependent on voluntary reports from doctors, who frequently fail to report bad outcomes.
The F.D.A. said it agreed that it needed a better system to detect harm to patients. By September 2016, the agency had received 285 reports of uterine cancer being spread by morcellation.
Amy Josephine Reed was born on March 22, 1973, in Bristol, Pa. Her mother, the former Joann Tunis, was a pharmacist and executive at the drug company Pfizer. Her father, William Reed, was a health insurance consultant.
Dr. Reed graduated from Pennsylvania State University in 1995 and went on to the University of Pennsylvania, where she earned a Ph.D. in immunology and a degree in medicine. She specialized in anesthesia and critical-care medicine.
She and Dr. Noorchashm met as graduate students and married in 2001. In 2011, both were offered teaching posts at the Harvard Medical School and clinical positions at its affiliated hospitals — Dr. Noorchashm at Brigham and Women’s and Dr. Reed at Beth Israel Deaconess. She treated victims of the Boston Marathon bombing in 2013, as well as the surviving bomber.
Besides Dr. Noorchashm, Dr. Reed is survived by her parents; her daughters, Nadia and Ava; her sons, Joseph, Joshua, Luke and Ryan; and seven siblings: Alison Perate, Andrea Kealy, Amber Trainer, Matthew Reed, Justin Reed, Daniel Trainer and Sarah Trainer.
https://mobile.nytimes.com/2017/05/24/us/amy-reed-died-cancer-patient-who-fought-morcellation-procedure.html?_r=0&referer=http%3A%2F%2Fm.facebook.com
Wednesday, September 23, 2015
FDA, Medical Device Industry Profit and Harmed Women Collide With Pope Francis in DC on September 24
Essure complaints spike nearly 1,400% in 3 years
SEPTEMBER 22, 2015 BY BRAD PERRIELLO
{kind=link}
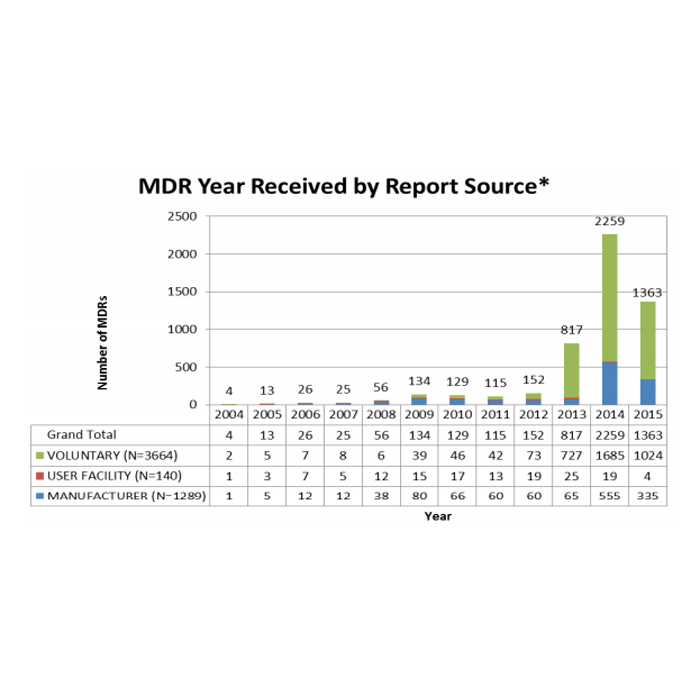
The FDA logged a nearly 1,400% spike in complaints filed over the Essure permanent female sterilization treatment made by Bayer (ETR:BAYN), according to a review released yesterday ahead of an FDA advisory panel meeting this week.
Essure, the only approved permanent birth control device in the U.S., is a small metal coil that is placed in the fallopian tubes via catheter. The FDA approved the device in November 2002.
In the near 13 years since then, the health regulator said it had received 5,093 complaints, including those of pain or menstrual irregularities after using the device, as well as complaints of the device breaking. Those adverse event reports include 5 fetal deaths in women who became pregnant after using Essure and 4 adult deaths for reasons such as infection and uterine perforation, the FDA said.
There were 152 complaints filed in the FDA’s Manufacturer & User Facility Device Experience database in 2012; last year there were 2,259 complaints filed in the MAUDE database, a 1,386% increase. So far this year there have been 1,363 MAUDE complaints filed with the FDA, the agency said. The FDA cautioned that the complaints it received had limitations such as incomplete or inaccurate data and did not necessarily directly indicate a faulty or defective device.

The FDA’s Obstetrics and Gynecology Devices advisory panel is set to meet Sept. 24 to discuss the risks and benefits of Essure and has invited feedback from presenters, panel members and the public. Some 17,000 women who had the device implanted and claim it has hurt them are members of the Facebook group “Essure Problems,” run by Angela Lynch, who herself experienced problems with Essure. Complaints voiced by the women include chronic pain, heavy bleeding, fatigue and skin allergies.
Lynch, who was 28 when she was implanted with the device, had 3 children and did not want any more.
“Because I had just had a kid I wrote off all my symptoms as hormonal, my body trying to adjust,” she said. “After 2 years I started losing hair. Then I started losing teeth, and over time it got to where my whole body was hurting.”
In 2012 she had the device removed and underwent a hysterectomy.
“After 3 days it was like I woke up from a 5-year flu,” she said.
In May, Bayer cited a 364-patient 5-year study of the device published in the Journal of Minimally Invasive Gynecology that indicated no pregnancies after 5 years and that the Essure inserts were “generally well tolerated.” Pelvic pain was reported in no more than 7% of patients, but no study participants reported persistent pelvic pain of any kind at the 3-, 4-, and 5-year follow-up visits, according to Bayer.
The study reported 3 serious adverse events “possibly related” to Essure in the trial, including irregular menstrual bleeding, lower abdominal pain and heavy periods and continuous bleeding. The latter 2 patients ended up having hysterectomies.
Dr. Patricia Carney, the company’s medical director for Essure, said Bayer welcomes the discussion. “We want to understand as a company what is going on,” she said. “We want to know whether there is a link to the product.”
In February a citizens petition lodged with the FDA asked the safety regulator to take Essure off the U.S. market, alleging that the clinical data the FDA used to approve the device was fudged and that the company concealed adverse events associated with Essure.
In July, the FDA approved using transvaginal ultrasound as an alternate test to confirm if the Essure implant has been placed properly. A month later Bayer cut the ribbon on a new plant in Costa Rica where it plans to make Essure.
Material from Reuters was used in this report.
http://www.massdevice.com/essure-complaints-spike-nearly-1400-in-3-years/
Monday, April 6, 2015
Thursday, June 6, 2013
Consumer App for Reporting Adverse Events to FDA!
Reporting Adverse Events?
There's an App for That, But Not for Industry--Yet
Need to report an adverse event
related to a medical device? Now patients are about to find there's an app for
that, US regulators revealed yesterday. https://medwatcher.org
Background
The US Food and Drug Administration
(FDA) takes in an enormous number of adverse event reports each year through
various systems, including MedWatch.
One issue, however, is that
manufacturers, healthcare providers and patients are held to different
standards. Medical device manufacturers, for example, are held to medical
device reporting regulations that require them to report to MedWatch any
adverse events they are made aware of, including for off-label uses.
Patients and healthcare providers,
meanwhile, are able to report adverse events, but are not required to do so.
That difference has led to significant under-reporting of
adverse events according to some estimates, posing a challenge for
regulators in their attempts to transition more of the regulatory assessment process to postmarket
settings. If, for example, a particularly dangerous adverse event is only seen
in one out of every 10,000 patients, it might not be picked up by clinical
testing. Once on the market, lax adverse event reporting practices by
healthcare providers could delay the time at which the company and regulators
become aware of that safety issue, potentially putting more consumers at risk
for a dangerous event.
A New App
That's where FDA's new MedWatcher adverse event reporting application
(iOS version)
(Android version)
comes in, said Bill
Maisel, deputy director for science and the chief scientist at FDA's Center for
Devices and Radiological Health (CDRH), in a statement.
"This app allows medical device users to easily report suspected or
known problems with a device from their smartphone or tablet," he said.
Users in this context include patients, caregivers, and healthcare
professionals, FDA explained.
Maisel later said in an interview
with the Wall Street Journal that the crux of the issue for FDA was:
"How can we all find out earlier than we have been finding out?"
"We'll get access to better data more quickly now," he
hypothesized.
The audience the application is not
to be used by is worth noting in this context: Medical device manufacturers and
healthcare providers. Maisel said that these two groups, "will continue to
be required to report problems through the Medical Devices Reporting System and
the Medical Product Safety Network."
Indicative of Future Changes?
But as Jeffery Shuren, director of
CDRH, said at the Medical Device Manufacturers Association's (MDMA) annual
meeting in April 2012, the system could be a harbinger of changes to come for
industry.
According to MD+DI's Arundhati
Parmar, Shuren said that the MedWatcher app "will push through
adverse events into the database that will replace the Manufacturer and User
Facility Device Experience (MAUDE)
database. “It would make it easier
for aggregating adverse event reporting.”
That functionality could eventually
lead to device manufacturers being given the same reporting capabilities as
consumers—an outcome that seems all the more likely given that the MedWatcher
app is basically just a more user-friendly version of FDA's Form 3500,
according to FDA.
"We're transforming this
network into a modern system that uses electronic health information,"
William Maisel confirmed in an interview with the Wall Street Journal.
But the idea of an app hasn't
received unanimous support. Paul Ivsin, a consulting director for clinical
trials, argued last week
that FDA would be better served by avoiding the use of apps entirely, and
instead focus on "developing a robust set of Application Programming
Interfaces (APIs) that can be used by the teams who are developing medical data
apps." That would result in a wider array of more customizable options to
meet the needs of hospitals, manufacturers and patients, he argued. In
addition, they could link up with other databases, such as the Sentinel
Initiative, giving users access to more information. That would also be in line
with a 2012 White House
directive ordering agencies to make more data open to the public via
APIs.
For now, though, FDA can only wait and see whether consumers
actually use the applications. As of the time of this article's publication,
the app has been downloaded more than 10,000 times.
Subscribe to:
Posts (Atom)